
Diranersen’s Gambit
Biogen sacrificed a clean endpoint and proved something bigger. The market will grade the tau question. The delivery question is the one that reprices the field.

Robert Toczycki, JD, MBA
bioboyscout.com
bioboyscout@gmail.com
847.227.7909
X: @BioBoyScout
Biogen presented the full Phase 2 CELIA results for diranersen at AAIC today, and by tonight every summary will have converged on the same question: does lowering tau treat Alzheimer’s disease. That is a fair question. It is not the one that moves the most value, and the gap between those two questions is where this note lives.
Two things were tested in that trial, not one, and only one of them is being talked about.
Two questions were on trial, not one
Think of a drug as a package that has to reach an address. The first question is whether the package arrives and does its job once it gets there. The second is whether that job actually helps the patient.
Those questions are worth very different amounts. A delivery answer travels. Prove that you can get a gene-silencing drug into the human brain and switch off a gene there, and you have opened the door for every drug that follows down the same road, whatever it aims at. An efficacy answer does not travel. Prove that lowering tau helps in Alzheimer’s, and you have proved exactly that, and nothing about the next target or the next disease. One answer opens a portfolio. The other adds a drug.
The market will grade the second question and shrug at the first. It has that backwards, and the rest of this note explains why.
What the data actually showed
Start with what was already public. In May, Biogen reported that CELIA missed its primary endpoint. The trial was supposed to show that higher doses worked better than lower ones, and it did not. Everything else, though, worked. Tau came down in the spinal fluid and, more impressively, tau came down in brain scans, at every dose, and it stayed down. Patients declined more slowly at every dose. The oddity: the best result came at the lowest dose, 60 mg given every 24 weeks, while the most serious side effects showed up at the highest dose. Biogen is pushing ahead to final-stage trials anyway.
Today’s presentation filled in the numbers, and they are better than the May summary implied. Tau in the spinal fluid fell by 50 to 65 percent across the dose arms by week 72, and tau also came down on brain scans in every brain region they looked at. No tau drug had ever moved both of those measures at once in a study this size. On the patient side, the winning dose slowed the decline of the disease by 26 percent, a difference of 0.54 points, on the main scale doctors use to track cognition and daily function, and by 42 and 50 percent on two pure memory-and-thinking tests. For scale, Leqembi, the amyloid drug already approved and on the market, slowed decline by 27 percent on that same main scale. A tau drug just matched an approved Alzheimer’s drug, and beat it on the thinking tests.
Then comes the detail almost no one will write about. Diranersen is injected into the spinal canal, a lumbar puncture, the same procedure people call a spinal tap. The three most common side effects in the whole trial were pain from the procedure, post-puncture syndrome, and confusion in the days right after dosing. Two of those three are the needle rather than the medicine, and the cleanest evidence for that is the placebo group: 57.9 percent of the patients who received no drug at all still had an adverse event attributed to the injection procedure. Fifty-eight percent, from the needle alone.
The third one, confusion, is more interesting, and it is not procedural. Every arm in the trial received an intrathecal injection every 12 weeks, drug or placebo, so the number of punctures was identical no matter which group a patient landed in. Confusion nonetheless grew more common the more drug a patient received. A side effect that tracks the dose cannot be caused by a procedure that does not vary with the dose. It is not the puncture. It is what the puncture delivers, and the concentration spike a bolus into the spinal fluid creates. Biogen also confirmed that this class does not carry the brain swelling and small bleeds that come with the amyloid drugs, because that risk belongs to the amyloid approach, not the tau one.
The full safety table adds something the May topline concealed. Harm climbed with dose while benefit did not. Side effects that Biogen’s own investigators judged related to the treatment affected 24.6 percent of the placebo group, then 37.7 percent at the winning low dose, 40.9 percent at the middle dose, and 57.8 percent at the highest dose, rising at every step. Serious side effects judged related to treatment ran from zero on placebo to 10.3 percent at the top dose, though not in a straight line, since the middle dose came in slightly below the low one. Set the exception aside and the shape is unmistakable. The most harm was concentrated in the arm that received the most drug, and Biogen’s own words for what that arm delivered in return were a lower effect size at the higher dose levels.
Figure 1: Level on the global scale, ahead on cognition, absent on function
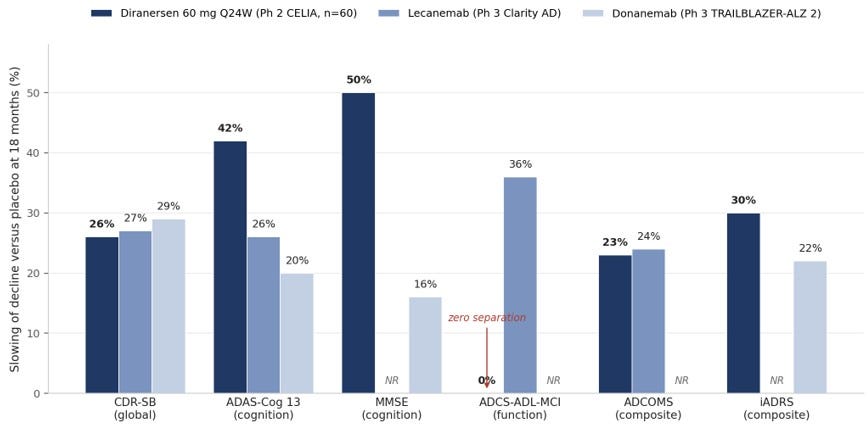
Slowing of decline versus placebo at 18 months, as compiled by Biogen. Diranersen figures are the 60 mg every-24-weeks arm from the Phase 2 CELIA study (nominal significance, 60 patients); lecanemab and donanemab figures are from their Phase 3 trials (roughly 900 patients each). NR indicates the endpoint was not reported for that trial. Cross-trial comparisons are illustrative, not head-to-head. Source: Biogen AAIC 2026 investor presentation, July 14, 2026.
How it stacks up against the amyloid drugs
The comparison everyone will want, and almost no one will run properly today, is diranersen against the approved amyloid antibodies. Run it carefully, because the honest version is more interesting than the cheerleading one.
Take the main scale first, the one regulators weigh most heavily, which measures cognition and daily function together. Diranersen slowed decline by 26 percent at its best dose. Leqembi slowed it by 27 percent. Kisunla, the other approved amyloid drug, managed 29 percent. The tau drug therefore landed level with both approved drugs on the measure that matters most. On the pure thinking-and-memory tests, the picture tilts. Diranersen slowed decline by 42 percent where Leqembi managed 26 percent and Kisunla managed 20 percent, and it produced a 50 percent effect on a standard memory test where Kisunla managed 16 percent. On the two composite scales that blend cognition and function, diranersen scored 23 percent on ADCOMS against Leqembi’s 24, and 30 percent on iADRS against Kisunla’s 22, the only scales on which each of those drugs reported. On cognition alone, the tau drug looks better than the drugs already on pharmacy shelves. Everywhere else, it looks like a peer.
There is one column where it does not look like a peer, and Biogen printed it without comment. On the standalone measure of daily functioning, the ability to manage money, drive, keep up hobbies, diranersen showed zero separation from placebo. Leqembi showed 36 percent on that instrument. Aducanumab, in the trial that worked, showed 42 percent. Zero is not a small number. Daily functioning is what families actually feel, and it is a large part of what regulators are buying when they approve an Alzheimer’s drug.
Biogen’s answer to that, and it is a real answer rather than a dodge, is that the functional subdomains inside the main scale did move. Community affairs slowed by 21 percent, home and hobbies by 24 percent, personal care by 29 percent. Two instruments measuring roughly the same thing disagreed, and the one Biogen highlighted is the one that agreed with the drug. That may be noise in a 60-patient arm. It may be a real gap between what a clinician observes and what a caregiver questionnaire captures. It cannot be waved away, and it is the single largest hole in the registrational case.
Four further caveats keep this from being a victory lap. This is a mid-stage result resting on 60 patients in the winning group, the smallest arm in a study that put nearly twice as many patients in each of the others, against late-stage trials with roughly 900 patients each, and effects of this kind shrink more often than they grow when the trial gets bigger. The brain-scan substudy at the winning dose rested on 19 patients at baseline and 16 at the end. The statistics behind diranersen’s numbers are softer, too, held to a looser standard than the approved drugs were. The winning arm also entered the trial carrying less amyloid and fewer double copies of the highest-risk Alzheimer’s gene than the arms it beat, which is the kind of imbalance that can flatter a result. In fairness, it cuts both ways: that same arm started with worse cognition and more advanced disease, which would ordinarily predict faster decline, not slower. Randomization did its job imperfectly in both directions, which is what happens when an arm has 60 people in it. No single trial settles a question like this.
The safety comparison runs firmly the other way, and it is the more durable advantage. The amyloid drugs can cause brain swelling and small brain bleeds. That risk brings the FDA’s strongest warning label, repeated brain scans to monitor for it, and a genetic test before treatment even starts. The tau approach does not carry that risk, and this trial confirmed it. Nothing in diranersen’s safety profile is a mechanism attacking the brain’s blood vessels. Its burden is the route and what the route delivers. Put those together and the strategic picture is clear. Tau is now a proven target rather than a theory, and the drugs competing to hit it will be separated by how they are delivered and how safe they are, not by whether the idea works. That is precisely the ground Arrowhead built ARO-MAPT to fight on.
The endgame is a combination, and that changes everything
Look at those two columns again. The amyloid drugs did better on daily functioning. The tau drug did better on thinking and memory. Those do not look like two drugs competing to do the same job. They look like two drugs doing different halves of one job.
The biology says the same thing. Alzheimer’s is a two-protein disease. Amyloid builds up first, tau follows, and tau is the one that tracks most closely with symptoms, the protein that tangles inside brain cells in the places where memory actually fails. Clearing amyloid alone treats the trigger and leaves the bullet in flight. Almost everyone in this field now expects the eventual answer to be both, an amyloid drug and a tau drug together, and Biogen happens to own one of each.
Here is what almost no one is saying about that. If combination therapy is the destination, then how a drug is delivered stops being a matter of convenience and becomes the thing that decides whether the destination is reachable at all. Build that combination out of the standard of care as it stood until this week and you get an intravenous infusion in a clinic every two weeks for eighteen months, then an infusion every four weeks after that, plus a lumbar puncture every six months, for the rest of a patient’s life. Burdens do not simply add when you combine therapies. They compound, because the patient has to accept all of it, the doctor has to schedule all of it, and the payer has to fund all of it. Two clinic-bound drugs is not twice as difficult as one. It is disqualifying.
The timing here is almost too neat. One day before this presentation, the FDA approved Leqembi Iqlik, a once-weekly subcutaneous autoinjector, as a starting dose for early Alzheimer’s, which makes lecanemab the first anti-amyloid therapy a patient can take at home from the first dose through maintenance. The Alzheimer’s Drug Discovery Foundation said out loud what the approval means: a step toward the scalable care model the disease will need as the field moves from single drugs toward combinations. The amyloid half of the future combination just left the infusion center. The tau half is still in it.
Now picture the combination built out of what exists after this week: an at-home autoinjector for the amyloid drug, alongside a tau drug given as a shot under the skin once a quarter. There is exactly one tau program in clinical development that fits that description, and it is Arrowhead’s ARO-MAPT. Diranersen cannot be that drug, because a spinal tap does not happen at home. Every anti-tau antibody that might have been that drug has already failed. The regimen an ordinary neurologist can prescribe and an ordinary patient can live with for years is amyloid by autoinjector plus tau by subcutaneous injection, and Arrowhead owns the only candidate for the second half of it.
Readers of my first paper, The Needle Wins, will recognize the argument, because this is that argument arriving in a new disease. The thesis there was that the auto-injector had already normalized self-administration for tens of millions of people, and that any therapy which could migrate into that format would capture a market that clinic-bound competitors could not reach. Alzheimer’s crossed that line yesterday. The needle wins in neurology too, and the drug positioned to benefit most from it is not the one that just won the tau argument.
Be honest about the caveats. No one has run the combination trial, so the benefit is a hypothesis rather than a result, the costs of stacking two branded biologics will meet real resistance from insurers, and the safety of combining them has to be established rather than assumed. ARO-MAPT has also not yet shown a single human data point. Grant all of that, and the strategic point still stands. The moment the field decides the future is combination therapy, the drug that can be given as a simple shot is not merely the more pleasant option. It is the only version of the future that actually works, and Arrowhead is the only company holding a tau asset built for it.
The finding nobody else will write about
The strangest result in the trial is the one most likely to be glossed over. The lowest dose worked best. Diranersen was tested at three dose levels, and the smallest one, given twice a year, beat both of the bigger ones on essentially every measure of patient benefit. That is why the study technically failed its main goal, which was to show that more drug produces more benefit. More drug did not.
The full data sharpens this into something stronger than the topline allowed. More drug did not merely fail to help. More drug did more of everything except help. The highest dose lowered tau the furthest in the spinal fluid, drove tau down the furthest on brain scans, produced the most treatment-related side effects, produced the most serious ones, and delivered the worst clinical result of the three. The lowest dose lowered tau the least of the three and helped the most. That is not a flat dose-response curve. That is an inverted one, running through both benefit and harm at the same time.
Figure 2: Harm scaled with dose. Benefit ran the other way.
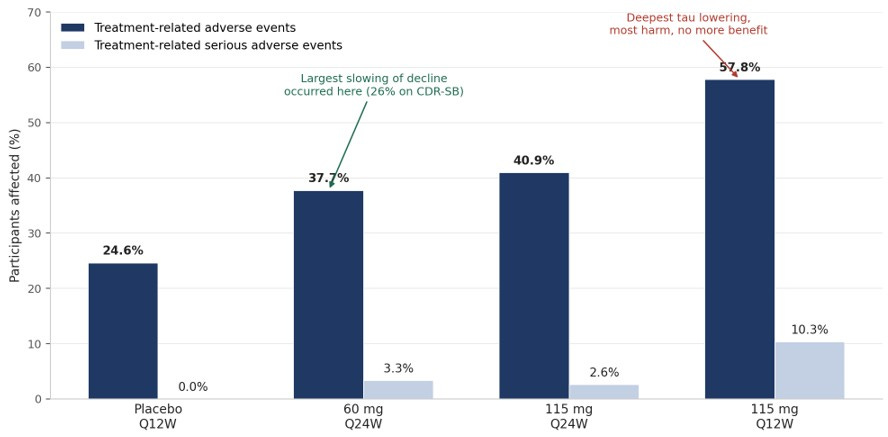
Treatment-emergent adverse events assessed by the investigator as related to study treatment, by randomized arm, from Biogen’s CELIA safety table (data cut 11 March 2026). Treatment-related adverse events rose at every step of the dose ladder. Serious treatment-related events rose from zero on placebo to 10.3 percent at the top dose, with a small non-monotonic dip at the middle dose. Clinical benefit ran the other way: the 60 mg every-24-weeks arm produced the largest slowing of decline on CDR-SB, and Biogen reports a lower effect size at the higher dose levels. Source: Biogen AAIC 2026 investor presentation, July 14, 2026.
There are two ways to read that, and the whole tau field turns on which one is true.
The first reading is biological. Tau is not purely a villain. Healthy brain cells use it for ordinary jobs, so stripping out too much of it may carry a cost of its own, and the curve turns down because the target itself has a floor. If that is right, the ceiling belongs to tau, and it applies to every drug that lowers tau, including Arrowhead’s.
The second reading is the needle. Harm rose monotonically with intrathecal exposure in Biogen’s own safety table, from zero treatment-related serious events on placebo to 10.3 percent at the top dose, with confusion specifically growing more common at higher doses. A drug that is helping a patient and injuring him at the same time will show exactly this curve, and the injury here is concentrated in events that trace to the route and to the peak concentrations a bolus into the spinal canal creates. If that is right, the ceiling belongs to the delivery, not to the target, and a route that reaches the brain gently and evenly does not inherit it.
Today’s data cannot separate those two readings, and any analyst who tells you otherwise is selling something. What it does establish is that the ceiling is real, that it arrived well below the doses Biogen tested, and that at least part of it is attributable to the way the drug gets in. Both readings converge on the same commercial conclusion. The winning technology in tau is not the one that hits hardest. It is the one that can hold a steady, moderate, precisely controlled reduction without paying an escalating toxicity toll to get there, which happens to be a description of what a quarterly injection under the skin is built to do.
The read-through to ARO-MAPT
The data landed on the most favorable branch available, and it landed on two of them at once. The mechanism worked and the route hurt.
Start with the mechanism. Deep tau knockdown produced a real cognitive signal, which validates tau as a target and, with it, the premise beneath Arrowhead’s ARO-MAPT. Someone else spent the capital to de-risk the target. Arrowhead inherits the benefit. The competitive question now narrows to delivery burden, and that is precisely where a subcutaneous injection has an obvious advantage over a repeat spinal tap.
Then the route. The winning regimen, 60 mg every six months, means two lumbar punctures a year, for life. Two of the three most common adverse events in the trial are the puncture itself, and the third is the concentration spike the puncture delivers. Every one of them is an argument for changing the route rather than changing the drug. The subcutaneous case no longer needs to be argued in the abstract. It is written into Biogen’s own safety table.
Steelman the other side, because there is a real counterargument and it appeared in this deck. Ninety-four percent of the patients who finished the study chose to continue into the extension, which means they signed up for years of further spinal taps. Patients tolerate the needle better than the delivery thesis assumes. Two honest responses. Clinical trial volunteers are the most motivated patients in the disease and are not the population that decides whether a drug reaches millions of people. Twice-yearly dosing is also genuinely less frequent than a quarterly subcutaneous injection, so the argument for a shot under the skin cannot rest on how often, only on what kind and where. The case is invasiveness and setting, not arithmetic, and it should be argued on those terms.
Where the route stops being a preference and becomes the whole game
Alzheimer’s is the largest tau market. It is not the market where delivery decides the winner, because in Alzheimer’s the two routes cover roughly the same ground. Tau pathology in Alzheimer’s begins in the entorhinal cortex and hippocampus and spreads through the association cortices, and those structures sit reasonably close to the fluid spaces that a spinal injection can reach. Diranersen’s 50 to 65 percent reduction in spinal fluid tau is evidence that intrathecal delivery gets to the places Alzheimer’s lives.
Now consider what today’s result opens up. CELIA validated tau lowering as a mechanism, not as an Alzheimer’s drug. The same mechanism points at a set of rarer diseases where tau is not one of two proteins but the only one: progressive supranuclear palsy, corticobasal degeneration, and the inherited frontotemporal dementias caused by mutations in the tau gene itself. None of them has an approved disease-modifying therapy. All of them are now more investable than they were yesterday, because the target has been reached and lowered in a human brain with a cognitive signal attached.
These are also the diseases that live in exactly the wrong part of the brain for a needle in the spine. Progressive supranuclear palsy is a disease of the subthalamic nucleus, the substantia nigra, the red nucleus, and the brainstem nuclei, including the structure whose degeneration produces the vertical gaze palsy that defines the illness. A drug injected into the lumbar spine travels up the fluid column and diffuses inward from the brain’s outer surfaces, so the structures nearest the fluid see the most drug and the structures buried deepest see the least. That gradient is a property of the route, not of the molecule, and no amount of chemistry improvement repeals it.
Look at what Biogen has published from its own animal work, and then at what it has not. Its intrathecal tau drug produced 77 percent knockdown in the frontal cortex and 74 percent in the hippocampus, which are precisely the structures the spinal fluid bathes most easily, and those are strong numbers. There is no published figure for the substantia nigra, and none for the brainstem. A program this far advanced, in a field this competitive, does not leave favorable data unpublished. The silence is the gradient. Arrowhead’s drug travels through the bloodstream instead, using a receptor expressed on the lining of brain blood vessels everywhere. Across 14 brain regions in primates, drug accumulation ran from 0.47 micrograms per gram in the substantia nigra to 1.55 in the motor cortex, a spread of roughly threefold, with the lowest region still above the threshold that produces knockdown. Arrowhead’s own slide put it plainly: the distribution overcomes the intrathecal limitation in deep brain delivery.
Hold the caveat firmly. That is a monkey, not a person, and the human distribution data does not exist yet in any program. Grant the caveat and the strategic shape is still unmistakable. In Alzheimer’s, the route is a commercial advantage. In the rare tauopathies, the route is the difference between a drug that reaches the disease and one that does not, and those are the indications with no competition, orphan pricing, and an accelerated regulatory path.
One more thing the route argument gains today. Arrowhead is not the only company that concluded the failures in tau were about getting there rather than about tau. Denali’s DNL628 uses the same class of receptor-mediated brain transport, delivered intravenously, with its first patient data expected in the first half of 2027. A third serious player betting on brain-crossing tau knockdown is corroboration of the thesis rather than a threat to it, and on the current timelines Arrowhead reads out first and is alone in the subcutaneous lane.
The number to grade the autumn on
The most useful thing to take from today is a bar, and it is now a precise one. Diranersen lowered total tau in the spinal fluid by 50 to 65 percent across the dose arms, and the arm that produced the clinical benefit sat at the shallow end of that range. Arrowhead’s management has said it is looking for a comparable reduction in its own healthy-volunteer study as the mark of success. The autumn readout now has a number rather than a mood, and the number is roughly half.
Arrowhead’s animal data already sits there. In primates, ARO-MAPT produced roughly 50 to 60 percent reductions in tau in the spinal fluid, holding for up to four months after the last dose, and its modeling projects sustained knockdown of 50 to 70 percent on quarterly dosing. My own translation framework, published before today, was more conservative than the company’s: 40 to 55 percent in humans at an optimal loading dose, with anything above 55 percent exceptional and anything below 30 percent a translation failure. That conservatism used to be a concession. Today it is a fit. Since the arm that produced the benefit sat at the shallow end of the band, a 40 to 55 percent human result for ARO-MAPT is not a disappointing near-miss of the benchmark. It lands in the range that worked.
Be clear-eyed about the flip side, because this is the real risk and it is quantitative rather than binary. The advantage of a shot under the skin only counts if the knockdown lands in the right range. Convenience does not rescue a weaker drug. If ARO-MAPT reaches the brain but silences only a fraction of what a spinal injection achieves, the delivery win is real and the commercial case is not. What today changed is the shape of the target. Arrowhead no longer has to beat diranersen on depth of knockdown, because depth of knockdown is not what won this trial. It has to land in the band, hold it steadily, and then win on everything else.
Set expectations correctly on what the autumn actually delivers. The readout coming in late September or October is the healthy-volunteer portion of the Phase 1/2a study. It answers whether a subcutaneous injection crosses into the human brain and lowers tau, and how much. It does not answer whether patients decline more slowly, because it does not enroll patients. Alzheimer’s patient data comes later, in 2027. Anyone expecting a cognitive result this autumn is going to be disappointed by a study that was never designed to produce one, and anyone who understands what is actually being tested will recognize it as the only question that has ever mattered for this program.
One practical note on timing
Expect the readthrough to be a slow burn rather than a same-day move. Arrowhead has its own topline coming in severe hypertriglyceridemia, the SHASTA readout, and that is the nearer and louder catalyst. JPMorgan made the point plainly: full credit for the tau work may only be realized on the back of that cardiometabolic topline. A tape focused on one readout does not price a second one that belongs to a competitor. The derisking today is real, and it will still be real in the autumn, when Arrowhead’s own brain data arrives and the market finally has to price it directly.
The gambit
Chess has a word for what Biogen just did. A gambit is a deliberate sacrifice, material given up on purpose to gain position. The player who offers it accepts a visible, immediate loss in exchange for something harder to see on the board: open lines, freer pieces, a position that pays out later.
Biogen sacrificed the endpoint. It gave up the clean win, a met primary and an unambiguous headline, and what it purchased with that loss was position for the entire field. Tau is now a target that has been reached, engaged, and lowered in the human brain, with a cognitive signal attached that matches the approved amyloid antibody. That knowledge did not exist in a randomized trial before today, and Biogen paid for it with a missed primary, an invasive route, and a dose curve that turned out to argue against its own higher doses.
Look closely at what Biogen is now proposing to do with the position. Its final slide says the data supports moving diranersen into registrational studies. Its next-steps slide commits to nothing firmer than continued engagement with regulators on Phase 3 planning, with no start date and, tellingly, no declared dose. The company intends to take the lowest dose, from the smallest arm, in a trial that failed the prespecified test of whether dose matters at all, into a program that will cost it hundreds of millions of dollars. That is the second half of the gambit, and it is the half that has not been paid for yet.
Here is the thing about a gambit, though. The player who sacrifices is not always the player who collects. A gambit opens a line, and whoever has a piece already trained on that line is the one who benefits from it. Biogen opened the tau file with a drug that has to go into the spine. Arrowhead is aiming down the same line with a shot under the skin, and it did not pay a dollar for the position it just inherited.
What it means
Today was a delivery win dressed up as an argument about tau. A drug reached the human brain, found its target, and cleared out tau, which is what this field has been chasing for a decade. Whether tau is the right thing to chase is a separate question, still open, and it will be settled in years of late-stage trials, not in a conference room in London.
The lesson for a platform investor is the one I keep returning to. Bet on the road, not on the destination. Targets fail, and they fail often. A validated way into the brain does not, and it can be pointed at the next target, and the one after that. Arrowhead’s own first human brain readout arrives later this year, and it should be judged on exactly the terms this note has laid out: can it get there, how much drug it takes, and how precisely the knockdown can be controlled. Whether it cures anything is a question for a different year.
Biogen made the sacrifice. The position is open. Watch who plays into it.
A Note on Supporting Independent Research
If this note has been valuable to you, whether it shaped your thinking, validated your conviction, or simply saved you the time of doing this work yourself, a voluntary contribution is genuinely appreciated and directly funds the next paper.
For individual investors and readers
Any amount you feel reflects the value you received is welcome and meaningful. A contribution in the range of what you might pay for a single premium research report is a thoughtful gesture that makes a real difference.
For family offices, investment funds, hedge funds, and research platforms
This paper is the caliber of work that institutional research desks bill significant retainers to produce. If your team referenced it, distributed it internally, or used it to inform a position, a suggested contribution of $1,000 reflects the professional value of the analysis, though any amount is meaningful. Your support makes it possible to continue publishing at this level without a paywall that limits the reach of the ideas. If your organization requires an invoice to process a payment, please reach out directly at bioboyscout@gmail.com and one will be provided promptly.
There is no obligation and no expectation. This is purely a thank you for work that meant something to you.
Zelle: (847) 227-7909
Thank you for reading, and for being part of a community that takes this thesis seriously.
— Robert Toczycki | BioBoyScout
Important Risks, Disclosures, & Disclaimers
The author, Robert Toczycki (aka BioBoyScout), certifies that:
all views expressed in this note accurately reflect his personal opinions about the topic discussed;
he was not compensated in any form for producing this note; and
he has not received and does not receive compensation from Arrowhead Pharmaceuticals.
This note reflects the author’s personal opinions, is for informational purposes only. It does not constitute investment advice, a solicitation to buy or sell securities, or a guarantee of future results. The author holds a long position in Arrowhead common stock. Arrowhead Pharmaceuticals (ARWR) is a publicly traded company; investments in its shares involve material risks, including the risk of total loss.
About the Author
Robert Toczycki is an independent analyst and registered US Patent Attorney with a JD, an Executive MBA completed at the top of his class, and a BS in Mathematics and Computer Science from the University of Illinois at Urbana-Champaign. He has a deep passion for financial analysis, particularly identifying valuation discrepancies and demonstrating them through rigorous, data-driven research and solid analytics.
Comments or questions: bioboyscout@gmail.com.
Copyright © 2026, BioBoyScout. All Rights Reserved.
Certainly much to unpack here. First off I would have liked to have seen the comparative P2 data for the approved amyloid mabs. Secondly, my company has not yet put forward a plausible explanation for the lack of dose-response (AFAIK). Thirdly, beyond superior safety (not trivial) and MOA advantages, I'd like to see some initiatives on patient segmentation (we may see this in the P3 trial design). If, ultimately combination therapy is the way to go, then we're going to need to see significantly larger changes on CDR-SB. Finally, as you stated there is clearly potential utility to use this approach in rare diseases such as PSP/CBD. However I can envisage potentially major pricing challenges (assuming clinical success-a big assumption) using the same drug both for rare and common neurodegenerative disease.