
Edit the Copy, Not the Original
The Investment Case for Reversible RNA Editing Over Permanent Gene Editing

A framework for when to silence a gene, when to correct it, and when permanent gene editing actually earns its risk, with case studies in cholesterol (PCSK9) and alpha-1 antitrypsin deficiency, and an investment lens on the companies that own reversible RNA editing.
Robert Toczycki, JD, MBA
bioboyscout.com
bioboyscout@gmail.com
847.227.7909
X: @BioBoyScout
I. Executive Summary
The thesis. Every genetic medicine, on the market or in development, does one of two things to a patient’s biology. It makes a temporary change that can be stopped, or it makes a permanent change that cannot. That single distinction, reversible versus permanent, is the most important and most underpriced idea in the field today, and it is the subject of this paper.
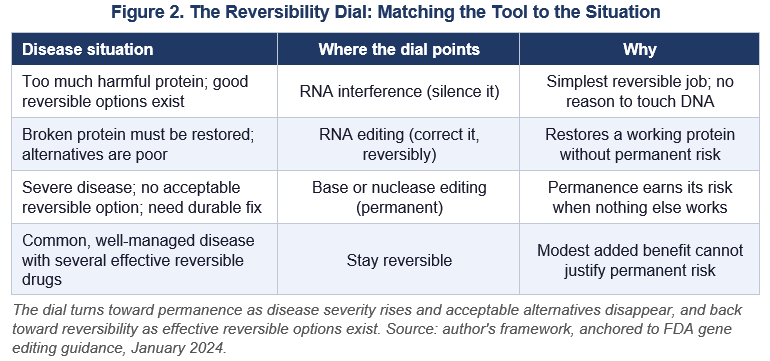
The framework. Reversibility is a premium, not a consolation prize. When a reversible medicine can do the job for a given disease, the permanent option must clear a much higher bar, because permanence carries one risk the reversible option never will: if something goes wrong years later, it cannot be undone. The right mental model is a dial rather than an on/off switch. The dial turns toward permanence as a disease grows more severe and acceptable alternatives disappear, and it turns back toward reversibility as effective reversible options exist. This framework is anchored to the language of the FDA’s own gene editing guidance, which recommends reserving irreversible, first-in-human treatment for patients who have no available or acceptable alternative.
The case studies. Two diseases anchor the argument at opposite ends of the dial. PCSK9, the cholesterol target behind Eli Lilly’s permanent gene editing program acquired with Verve, sits at the wrong end: it is the most crowded target in cardiology, already served by statins, antibodies, and the twice-yearly reversible therapy inclisiran. The adherence problem that gene editing claims to solve has already been attacked reversibly, the residual gap is operational with further unused fixes such as a mailed home autoinjector, and the modest convenience of a single treatment cannot justify a permanent, irreversible change. Alpha-1 antitrypsin deficiency sits at the right end: its alternatives are poor, and a single mutation damages two organs in opposite ways, a problem only correction, not silencing, can address. Reversible RNA editing now does exactly that in humans, at protein levels associated with protection.
The investment view. If reversible correction is where a meaningful part of genetic medicine is heading, the investment question is who owns the rails. ProQR, a small Dutch company, holds the foundational, opposition-tested patents on the kind of RNA editing that performs this correction, which makes it a potential toll booth on the entire modality. Wave Life Sciences leads the clinic, having delivered the first human proof of RNA editing, and it may need to license rights from ProQR. The clearest confirmation that the framework is real comes from the demand side: Lilly owns both the permanent editing program and a reversible RNA editing collaboration with ProQR, treating the two not as rivals but as a portfolio matched to the disease.
The risks. The thesis carries real risks worth stating plainly. RNA editing is clinically young, with far less long-term human data than established gene silencing. ProQR’s broad patents could be narrowed or invalidated. Strong early gene editing data, combined with an FDA posture that increasingly favors acceleration, could overrun the alternatives argument in the marketplace regardless of its merits. The reader should weigh the framework against the possibility that momentum, not logic, decides the near term.
II. A Plain-Language Primer: Four Ways to Change a Gene
Start with a kitchen. To follow the argument, you only need one analogy, and it holds up surprisingly well.
Think of your DNA as a master cookbook locked in a vault. It contains every recipe your body knows how to make. When a cell wants to cook one dish, it does not drag the whole cookbook out. It makes a quick photocopy of the single recipe it needs. That photocopy is called RNA. The cell follows the photocopy to make the dish (a protein), then throws the photocopy away and makes a fresh one next time. The master cookbook in the vault never moves.
A genetic disease is usually a typo. Somewhere in the cookbook, one letter is wrong, so the photocopy is wrong, so the dish comes out wrong or even poisonous. There are four ways to deal with that typo, and they differ in one decisive way: whether you touch the disposable photocopy or the permanent cookbook.
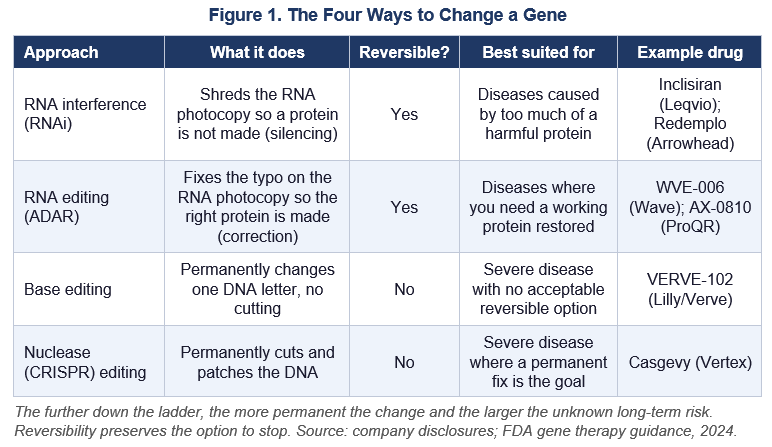
Option one, RNA interference (RNAi), is silencing. This shreds the bad photocopy before the cell can cook from it. The dish simply does not get made. The master cookbook is untouched, and the moment you stop the medicine, the cell goes back to making photocopies as before. This is what Arrowhead Pharmaceuticals and Alnylam do. Inclisiran, the cholesterol drug also known as Leqvio, works this way, as does Arrowhead’s alpha-1 drug fazirsiran. It is fully reversible.
Option two, RNA editing, is correction. Instead of shredding the photocopy, this fixes the typo on the photocopy itself, so the dish comes out right. It does this by recruiting a tool the cell already owns, a natural spell-checker enzyme called ADAR, and pointing it at the exact letter that needs changing. Because you are only editing disposable photocopies, the change fades when you stop dosing. The master cookbook is still untouched. This is what Wave Life Sciences and ProQR do. It is also fully reversible.
Option three, base editing, is a permanent single-letter rewrite. Now you are no longer touching photocopies. You are walking into the vault and changing a single letter in the master cookbook itself. Modern base editing does this cleanly, changing one letter without cutting the book. Every photocopy from then on is correct, forever, after a single treatment. This is what Verve Therapeutics, now owned by Eli Lilly, does to the PCSK9 cholesterol gene. It is permanent. You cannot undo it.
Option four, nuclease (CRISPR) editing, is a permanent cut and patch. This is the original CRISPR approach. It cuts the cookbook at the target spot and lets the cell patch it. It is powerful, but cutting the book is a bigger disruption than changing one letter, and like base editing it is permanent. This is what the approved sickle cell therapy Casgevy uses.
Figure 1 lays the four side by side. The pattern to notice is simple and runs through the whole paper: as you move down the ladder, the change becomes more permanent, and the amount of unknown, long-tail risk goes up with it. Reversible options let you stop if something surprising shows up years later. Permanent options do not.
III. The Dial, Not the Switch: A Framework
How to choose. Two questions decide which rung of the ladder a given disease should use.
The first question is what job needs doing. If the problem is too much of a harmful protein, silencing it (RNAi) is enough. If the problem is a missing or broken protein that must be restored, you need correction (RNA editing) or a permanent rewrite (gene editing), because shredding photocopies cannot manufacture a working protein. Silencing and correcting are different jobs.
The second question is what alternatives already exist for that specific disease. This is where reversibility earns its premium. Reversibility is, in plain terms, the ability to change your mind. That ability is worth the most precisely when you know the least, and genetic medicine is young. We do not yet have decades of data on what a permanent edit does twenty or thirty years out. A reversible medicine lets a patient and doctor course-correct if a late problem appears. A permanent one does not offer that exit.
An analogy from chess. Chess players respect this instinct. The pawn is the only piece that can never move backward, so a careful player commits one only when the position leaves no better option, and keeps every other piece free to maneuver. A reversible medicine is a piece that can be repositioned. A permanent gene edit is a pawn that can never be called back.
What the FDA actually says. Regulators understand this. The U.S. Food and Drug Administration, in its January 2024 guidance on gene editing products, addresses exactly this point in its section on who should be enrolled in the first human trials. Because these products carry significant risks and uncertain benefits, the agency recommends that first-in-human gene editing trials generally enroll only patients for whom no other treatment option is available or acceptable. In plain terms: try the permanent, irreversible thing first on people who have nothing else that works.
Three details matter, and the paper will hold to them honestly. The recommendation is nonbinding guidance, not law. It applies specifically to first-in-human trials, not to the eventual marketed population. The phrase is available or acceptable, not merely available, which leaves room for argument about patients who have options on paper but are not well controlled by them. Even with those caveats, the principle is clear and it is the FDA’s own: irreversible risk should be reserved for situations where the alternatives have run out.
Put the two questions together and you get a dial, shown in Figure 2. It is not a ban on gene editing. It is a way to ask, for any given disease, how far toward permanence the situation actually justifies going.
IV. The Wrong End of the Dial: PCSK9 and One and Done
What is at stake. PCSK9 is a gene that raises LDL cholesterol, the bad kind tied to heart attacks and strokes. Turn PCSK9 down and LDL falls. People born with naturally low PCSK9 have low cholesterol for life and are strongly protected from heart disease. That genetic fact is the inspiration for trying to switch the gene off permanently.
What Verve and Lilly have. Eli Lilly acquired Verve Therapeutics in 2025 for roughly one billion dollars to obtain VERVE-102, a base editing medicine that permanently turns off PCSK9 in the liver with a single infusion. The early data are genuinely good, and this paper will not pretend otherwise. In the Heart-2 study reported in May 2026 and published in the New England Journal of Medicine, a single dose reduced PCSK9 by up to 88 percent and LDL cholesterol by up to 62 percent, with the effect lasting, no serious treatment-related adverse events, no dose-limiting toxicities, and no discontinuations to date. Lilly plans to begin a Phase 2 study by the end of 2026 and has built in 15 years of long-term safety follow-up.
In short, the science works. The question this paper raises is not whether it works. It is whether permanently editing a person’s DNA is the right tool for this particular disease, and the answer turns on the alternatives.
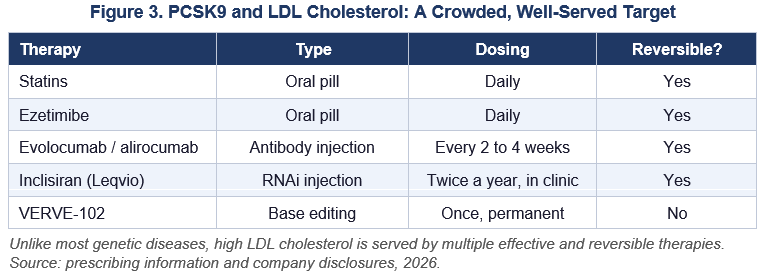
The crowded field. PCSK9 is the most crowded target in all of cardiology. A patient with high cholesterol already has a deep bench of effective, reversible options, shown in Figure 3. This is the opposite of a disease where the alternatives have run out.
Verve’s best argument: adherence. Verve’s strongest argument is not really about cholesterol numbers. It is about adherence. In the real world, patients stop taking chronic medicines. They miss doses, they quit within a year, and a drug that half of patients abandon prevents fewer heart attacks than its clinical trial suggests. A one-and-done treatment, the argument goes, cannot be abandoned, because there is nothing left to keep taking. This is a serious argument, and it deserves a serious answer rather than a dismissal.
The rebuttal. Here is the answer. The adherence problem in this drug class has already been attacked, reversibly, and the attack is on the market. Inclisiran is given as an injection twice a year, administered in a clinic by a provider. A patient cannot forget a medicine they do not self-administer and receive only every six months. Before reaching for a permanent edit to solve adherence, we should first ask how well the reversible twice-yearly option already solves it.
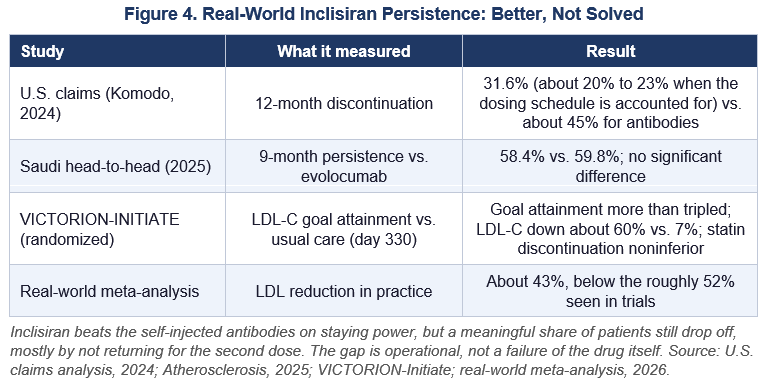
The honest answer, from real-world data, is that it helps a lot but does not fully solve the problem, and the exact numbers matter because they cut both ways. Figure 4 collects the main studies. A large U.S. claims analysis found that about 20 to 32 percent of inclisiran patients discontinued within a year, depending on how a missed dose is counted, compared with roughly 45 percent for the every-two-week antibodies. One head-to-head real-world study in Saudi Arabia found inclisiran persistence at nine months of about 58 percent, statistically no different from the antibody it was supposed to beat. The common drop-off point is the second dose at around day 90, which tells you the residual problem is patients not returning for an appointment, not patients forgetting a pill.
What this means. The claim that a reversible twice-yearly shot has fully solved adherence is therefore false, and this paper will not make it. Notice, though, what the residual problem actually is: people not showing up for an appointment. That is an operational problem, fixable with reminders and by folding the injection into routine visits, and it is fixable without permanently editing anyone’s DNA.
The unused lever: a home autoinjector. There is a further reversible fix that has not even been tried yet. Today, inclisiran is supplied as a prefilled syringe and is given in a clinic by a healthcare provider, and Novartis has promoted that twice-yearly, provider-administered model as itself an adherence feature, on the logic that the clinic, not the patient, controls the dose. The trouble is that this same design is exactly why the main drop-off happens when patients do not come back for the second visit. The obvious answer is not a permanent edit. It is a home autoinjector, a prefilled pen mailed to the patient, which is the very delivery model that GLP-1 medicines for obesity and diabetes have normalized for tens of millions of people. The technology is straightforward, because inclisiran is already a subcutaneous injection placed in the abdomen, upper arm, or thigh, the same route and sites those pens use. A patient who self-injects twice a year at home cannot miss a clinic appointment, because there is no appointment to miss. To be precise, no such home autoinjector for inclisiran is approved today, which is the point: it is an available, low-risk lever that has not yet been pulled.
The principle. The broader principle matters more than the single example. The reversible side of this contest still has several low-risk levers to close the adherence gap: the clinic model, a mailed autoinjector, appointment reminders, telehealth follow-up, or some combination of them, none of which requires changing a single letter of anyone’s DNA. When a problem can still be attacked with reversible tools that have not even been fully deployed, reaching first for the one tool that is permanent and cannot be undone is the weakest possible justification. The existence of unused reversible options is itself an argument against jumping to permanence.
The asymmetry. The decisive point is the trade itself. The extra benefit of a permanent edit over an already-good reversible option is real but modest: it closes a 20-to-30-percent adherence gap and spares a twice-yearly visit. The extra risk is categorical: you can never stop it. If a rare off-target effect or a slow problem appears years later, a reversible drug can be discontinued, and a permanent edit cannot. Modest extra benefit cannot buy categorical, permanent, irreversible risk. That asymmetry is the heart of the case.
The monitoring contradiction. There is a sharper version of the argument that uses Verve’s own premise against it. The FDA recommends up to 15 years of safety monitoring after a gene edit, to catch off-target and long-term effects. Now hold two claims together. Verve says these patients are too unreliable to keep taking a medicine. The 15-year monitoring plan assumes these same patients will reliably return for a decade and a half of follow-up. Both cannot be true. The patient too non-adherent for a twice-yearly injection is the worst possible candidate for 15 years of mandatory monitoring. Editing does not rescue the non-adherent patient. It gives them a single permanent change and then loses them to follow-up exactly as a prescription would lapse, except now there is an unmonitored permanent edit instead of a refill someone can simply restart.
The lifetime-exposure point. One more deflation. Verve’s grander pitch is that a permanent edit mimics being born with low PCSK9, and therefore delivers lifelong protection that a drug started in midlife cannot. The edit, however, is given to a middle-aged adult who has already accumulated decades of cholesterol exposure and, often, existing plaque. It does not reach back and undo those years. The real advantage over inclisiran, then, is not lifelong protection an injection cannot match. It is, once again, skipping the injections. The lofty framing collapses back into the convenience claim, and convenience cannot carry permanence.
Where Verve is right. Now the concession that makes the rest credible. There are real patients for whom one and done is not about convenience at all. People with the severe inherited form (homozygous familial hypercholesterolemia), patients dependent on blood-filtering apheresis, and patients in settings where returning every six months is genuinely not realistic, are cases where a durable single treatment can be a matter of survival, not comfort. For them the dial points toward permanence, and this paper concedes that cleanly. The argument has never been that gene editing should not exist. It is that the justification is strong at the severe end and grows weak as the target population widens toward ordinary, well-managed cholesterol.
The verdict. The concern, then, is not the drug. It is indication creep: the steady widening of an irreversible treatment from the severe patients who need it toward the large, well-served population who do not. The right posture is vigilance about that drift, not outrage at the medicine.
V. The Right End of the Dial: Alpha-1 and Why Fixing Beats Silencing
The textbook case. Alpha-1 antitrypsin deficiency, or AATD, is the cleanest illustration of why correction can beat silencing, and why the dial sometimes points decisively toward reversible RNA editing.
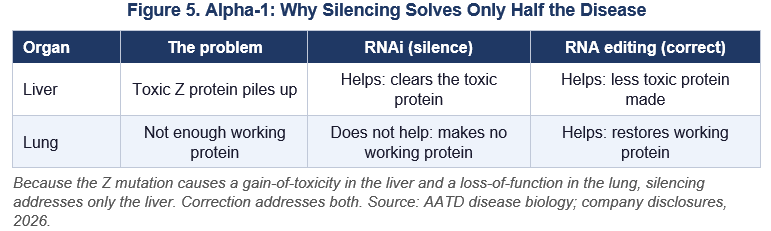
One typo, two opposite problems. AATD is caused by a single-letter typo in one gene, called the Z mutation. The remarkable thing is that this one typo causes two opposite problems in two different organs. In the liver, the misfolded protein piles up and becomes toxic; this is a problem of a harmful protein being present, a gain of bad function. In the lungs, the body lacks enough of the working protein that normally protects lung tissue; this is a problem of a good protein being absent, a loss of function. One typo, two opposite diseases.
Why silencing solves only half. This is exactly where the difference between shredding the photocopy and fixing it becomes decisive. Silencing (RNAi) shreds the photocopy of the bad gene. That clears the toxic protein out of the liver, which genuinely helps the liver. Shredding, however, cannot manufacture the good, working protein the lungs need. Silencing therefore solves the liver half of the disease and does nothing for the lung half. Figure 5 shows the split.
An honest note on Arrowhead. A point of intellectual honesty is required here, because the leading silencing drug for AATD is fazirsiran, which is Arrowhead’s own program, partnered with Takeda, and the author of this paper is long Arrowhead. Fazirsiran is a genuinely important and validated treatment. Before it, AATD liver disease had essentially no option but transplant, and fazirsiran addresses that real unmet need. The lung limitation described above is not a criticism of the drug or of Arrowhead’s execution. It is a property of the silencing approach applied to this particular two-sided disease. A fair framing presents fazirsiran as the validated liver treatment and notes the structural ceiling, rather than hiding either.
Why fixing wins here. Now the other side of the dial. RNA editing does not shred the photocopy; it fixes the typo, turning the bad Z protein back into the normal, working M protein. Conveniently, the Z mutation happens to be exactly the kind of single-letter change the ADAR spell-checker can reverse. Because you are restoring a working protein, you help both organs with one medicine, and because you are only editing disposable photocopies, the treatment stays reversible.
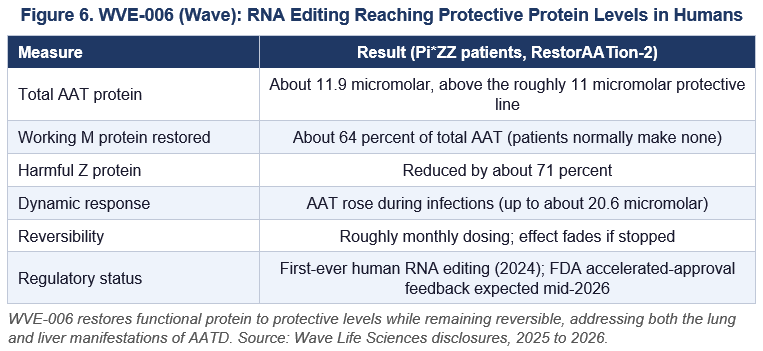
What Wave has shown. Wave Life Sciences has shown this in humans with WVE-006, partnered with GSK. In 2024 it became the first-ever RNA editing medicine to work in people, with the data deepening through 2025 and 2026. The numbers, in Figure 6, are not just a mechanism demonstration; they clear the level of protein associated with protection. Patients reached total AAT around 11.9 micromolar, above the roughly 11 micromolar protective threshold, with the newly produced working M protein making up about 64 percent of the total and the harmful Z protein cut by about 71 percent. The effect was sustained, dosing is roughly monthly and therefore reversible, and the body even raised its AAT output during infections, a dynamic, on-demand response that a fixed-dose protein infusion cannot match.
Why the dial points here. In AATD the alternatives are genuinely poor. The only approved treatment for the lung disease is weekly intravenous infusions of the protein (augmentation), a heavy burden, and the only option for advanced liver disease has been transplant. With alternatives that thin and a disease that needs a working protein restored in two organs at once, the dial points decisively toward reversible correction. This is the indication that proves the framework is not anti-editing. It is pro-fit: it sends each disease to the rung of the ladder that actually suits it.
VI. The Toll Booth: Who Owns RNA Editing
The investment angle. If reversible correction is where a meaningful slice of genetic medicine is heading, the investment question becomes: who owns the rails everyone has to run on? The answer points to ProQR.
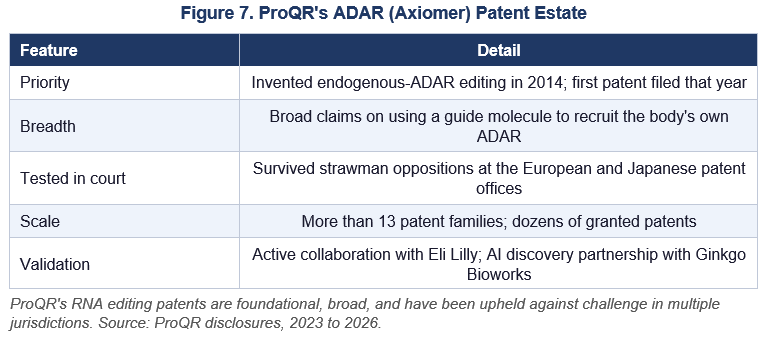
ProQR’s position. ProQR invented the core idea of recruiting the cell’s own ADAR spell-checker with a guide molecule back in 2014, and filed its first patent that same year. Its broad U.S. patent covers, in effect, using any guide molecule that recruits the body’s own ADAR to make this kind of edit. Crucially, the breadth has been tested rather than merely granted: ProQR has beaten anonymous challenges (known as strawman oppositions) at both the European and Japanese patent offices, and its estate now spans more than a dozen patent families and dozens of individual patents. Patents that have survived determined attack are a far stronger moat than patents that have simply been issued. Figure 7 summarizes the estate.
The Wave question, stated carefully. Now the most important and most carefully stated claim in this section. Wave’s WVE-006, the alpha-1 success story, works by recruiting the body’s own ADAR, which is the very activity ProQR’s broad claims describe. On its face, that means Wave may need to license ADAR rights from ProQR. The emphasis belongs on may. There are three honest possible outcomes, and no one outside the parties knows which holds: Wave may have designed around ProQR’s specific claims, Wave or its partner may be able to invalidate them, or there may already be a licensing arrangement that has not been disclosed. The strongest counterweight is that GSK, Wave’s deep-pocketed partner, did its freedom-to-operate homework before committing 170 million dollars upfront and up to 525 million dollars in milestones for the alpha-1 program, which means it reached some conclusion on this question that it found acceptable.
The risk. The risk to ProQR’s side is the mirror image of its strength. The same breadth that makes the claims valuable also makes them a target. Broad claims invite invalidity challenges, academic work in the field predates some of the claims, and a serious challenge in the United States has not yet been resolved. A reader should treat the licensing question as open and as optionality, not as a settled infringement finding.
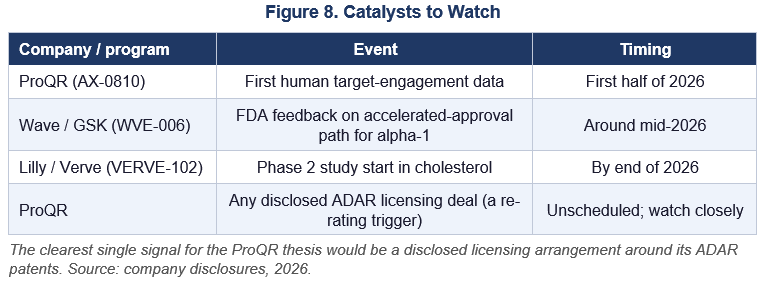
The reality check. A plain reality check keeps the thesis honest. Wave, not ProQR, leads the clinic in RNA editing today; ProQR’s own lead program, AX-0810, is only at the earliest stage of human testing, with initial target-engagement data due in the first half of 2026. In addition, RNA editing can only make certain letter changes, so it is not a universal fix. The ProQR case is therefore an intellectual-property and platform case, the toll booth on a road others are paving, not a claim that ProQR has the best drug in the clinic.
VII. The Tell: Lilly Owns Both Horses
Follow the money. The cleanest evidence that the reversible-versus-permanent framework is real comes not from any argument in this paper but from the behavior of the largest buyer in the field.
Eli Lilly owns Verve, the permanent PCSK9 editing program, and also has an RNA editing collaboration with ProQR, the reversible approach. The single most important company in the space is deliberately hedging across the exact line this paper draws. That is not a contradiction on Lilly’s part, it is portfolio logic. Lilly is betting that permanence and reversibility are not rivals to be chosen between, but different tools matched to different diseases, which is precisely the dial. When the biggest player treats your framework as its acquisition strategy, the framework is not a thesis anymore, it is the market structure.
VIII. The Drifting Standard
A tension worth naming. The framework has a complication on the regulatory side that an honest paper has to put on the table, because it cuts against the argument as much as for it.
What the guidance says. On one hand, the FDA’s written guidance encodes real caution. It reserves first-in-human gene editing for patients with no available or acceptable alternative, and it reserves its fastest approval lane, accelerated approval, for serious or life-threatening diseases that lack available alternatives. Read literally, that restriction does work against permanent editing in a crowded, well-served target like broad-population cholesterol, because such a population is hard to describe as lacking alternatives.
What the agency does. On the other hand, the agency’s posture in practice has leaned hard toward acceleration. Peter Marks, who ran the relevant FDA center until his resignation in March 2025 and was the field’s most prominent champion, publicly described base editing as a potential game changer, not only for rare diseases but for more common ones. He did note that as gene therapy moves toward common diseases, the FDA and payers may prefer traditional approval over the fast lane. Industry, for its part, pushed back on any hint that gene editing should face a higher hurdle, and the agency accommodated rather than doubled down. The leadership that followed has leaned further into speed.
On the word convenience. The honest read is that the caution in the FDA’s own guidance is in tension with the FDA’s own acceleration agenda. That makes the critique here one about a drifting standard, not about a villainous company. It also disciplines the argument in one specific way worth stating plainly. The FDA has not said that convenience can never justify approval, and it would be wrong to claim it did. Better adherence is a real, recognized clinical benefit, not a mere comfort. The defensible point is narrower and stronger: improving adherence is a benefit, but a modest one when a reversible twice-yearly option already exists, and the agency’s own pathway design reserves its fastest lane for serious, no-alternative diseases, which leaves broad-population editing to clear the longest, hardest path, full traditional approval on hard cardiovascular outcomes, the very evidence the reversible alternatives already carry.
IX. What to Watch, and What It Means for Investors
The catalysts. Several near-term events will test this framework in public, and they are worth tracking together rather than one at a time. Figure 8 lists the main ones.
Implications, stated as considerations. The following are factual considerations for a reader’s own analysis, not recommendations, and the author is not a financial advisor.
The reversible modalities, RNAi and RNA editing, are the category with the more forgiving risk profile and, in many diseases, the better fit, because they preserve the option to stop. ProQR is the intellectual-property toll booth on RNA editing if its claims hold, with the licensing question as the key swing factor. Wave is the clinical leader in ADAR editing today and the company that has put the first human proof on the board. Arrowhead remains the leader in RNAi, and its alpha-1 drug fazirsiran is a validated liver treatment; the lung limitation in AATD is a feature of the silencing approach for that disease, not a company-specific weakness.
Risks to the thesis. Several stand out, and each deserves honest weight. RNA editing is clinically young, with far less long-term human data than RNAi. ProQR’s broad claims could be narrowed or invalidated, which would deflate the toll-booth case. Strong VERVE-102 data combined with the FDA’s acceleration agenda and payer interest in one-time treatments could simply overrun the alternatives argument in the marketplace, regardless of its merits. A reader should weigh the framework against the possibility that momentum, not logic, decides the near term.
X. Conclusion
Reversibility is a premium, not a consolation prize. When a reversible medicine can do the job, a permanent edit must clear a much higher bar, because permanence carries one risk nothing reversible does: it cannot be undone, and in a field this young, the ability to change your mind is worth a great deal.
PCSK9 is the wrong end of the dial. It is the most crowded target in cardiology, its adherence problem has already been attacked reversibly and has obvious reversible fixes still unused, such as a mailed home autoinjector of the kind GLP-1 medicines made routine, the extra benefit of permanence is modest, and the patients least likely to stay adherent are the least suited to fifteen years of mandatory post-edit monitoring. Alpha-1 antitrypsin deficiency is the right end. Its alternatives are poor, it needs a working protein restored in two organs at once, and only correction, not silencing, can do that, which reversible RNA editing now does in humans at protective levels.
The companies that own reversible correction sit on the right side of that line: ProQR on the patents, if they hold, and Wave in the clinic. The clearest confirmation comes from the biggest buyer: Eli Lilly owns both the permanent horse and the reversible one, treating the dial not as a debate but as a portfolio. The question for the field, and for investors, is not whether gene editing should exist. It is how far down the severity gradient permanence should be pushed before the trade stops making sense, and on the evidence today the field is pushing it too far, too fast, for diseases that do not need it.
Chess offers the right picture to close on. The pawn is the only piece that can never move backward, which is why a careful player pushes one only when the position truly demands it. Gene editing is the pawn move of genetic medicine: sometimes necessary, always permanent, and never worth spending on mere convenience. Right now the field is pushing pawns to save a tempo it has not lost. The smartest move, in medicine and in markets alike, is the one you can still take back.
Appendix A. Glossary
ADAR. The body in your DNA’s master cookbook analogy. A natural spell-checker enzyme that the body already makes, which RNA editing recruits to fix a single letter on an RNA photocopy.
Base editing. Permanently changing a single DNA letter without cutting the DNA. Used by VERVE-102. Not reversible.
Nuclease (CRISPR) editing. Permanently cutting and patching DNA at a target site. The original CRISPR approach. Used by Casgevy. Not reversible.
LDL cholesterol. The bad cholesterol most tied to heart attacks and strokes.
PCSK9. A gene that raises LDL cholesterol. Turning it down lowers LDL.
RNA interference (RNAi). Shredding the RNA photocopy so a protein is not made. Silencing. Reversible. Used by inclisiran and fazirsiran.
RNA editing. Fixing the typo on the RNA photocopy so the right protein is made. Correction. Reversible. Used by Wave’s WVE-006 and ProQR’s Axiomer.
Alpha-1 antitrypsin deficiency (AATD). A genetic lung and liver disease caused by one typo (the Z mutation) that creates two opposite problems: toxic protein in the liver and too little working protein in the lung.
Adherence and persistence. Whether a patient keeps taking a medicine as prescribed over time. Persistence is the share still on treatment after a set period.
Appendix B. Sources
All figures and data points draw on the public sources below, each linked to its canonical page. Quotations have been avoided in favor of paraphrase; figures cite their sources in the captions above.
1. Eli Lilly and Company. VERVE-102 Heart-2 Phase 1b results, investor release, May 25, 2026. https://investor.lilly.com/news-releases/news-release-details/single-dose-lillys-pcsk9-base-editor-verve-102-reduced-pcsk9-88
2. In Vivo Base Editing of PCSK9 with VERVE-102 for Hypercholesterolemia. New England Journal of Medicine, May 25, 2026. https://www.nejm.org/doi/full/10.1056/NEJMoa2601283
3. Eli Lilly and Company. Completion of the acquisition of Verve Therapeutics, investor release, July 25, 2025. https://investor.lilly.com/news-releases/news-release-details/lilly-completes-acquisition-verve-therapeutics-advance-one-time
4. Verve Therapeutics. Lilly to acquire Verve Therapeutics; terms of about 1.0 billion dollars at closing and up to about 1.3 billion dollars with the contingent value right, June 17, 2025. https://vervetx.gcs-web.com/news-releases/news-release-details/lilly-acquire-verve-therapeutics-advance-one-time-treatments
5. Wave Life Sciences. First-ever therapeutic RNA editing in humans achieved in the RestorAATion-2 trial of WVE-006, October 16, 2024. https://ir.wavelifesciences.com/news-releases/news-release-details/wave-life-sciences-announces-first-ever-therapeutic-rna-editing
6. Wave Life Sciences. RestorAATion-2 update, 200 mg and 400 mg cohorts of WVE-006, September 3, 2025. https://ir.wavelifesciences.com/news-releases/news-release-details/wave-life-sciences-announces-positive-update-ongoing
7. Wave Life Sciences. RestorAATion-2 update, MZ-like phenotype across biweekly and monthly dosing of WVE-006, May 18, 2026. https://ir.wavelifesciences.com/news-releases/news-release-details/wave-life-sciences-announces-positive-update-restoraation-2
8. ProQR Therapeutics. Successful defense of patent EP 3234134 B1 at the European Patent Office against two strawman oppositions, March 14, 2023. https://www.proqr.com/press-releases/proqr-announces-successful-defense-of-a-key-axiomerr-patent-protecting-adar-mediated-rna-editing
9. ProQR Therapeutics. Japanese Axiomer patent JP 7244922 upheld after opposition; estate then exceeding 13 patent families and 27 patents, February 15, 2024. https://www.proqr.com/press-releases/proqr-announces-japanese-axiomertm-patent-upheld-following-opposition-against-its-leading-ip-estate-for-adar-mediated-rna-editing
10. ProQR Therapeutics. Successful defense of patent EP 3507366 B1 at the European Patent Office, April 19, 2024. https://www.proqr.com/press-releases/proqr-achieves-successful-defense-of-new-challenge-to-its-axiomertm-ip-portfolio
11. ProQR Therapeutics. AX-0810 Phase 1 safety and pharmacokinetic data, 2026 outlook, and Eli Lilly collaboration milestones; target-engagement data expected in the first half of 2026, January 8, 2026. https://www.proqr.com/press-releases/proqr-announces-encouraging-ax-0810-phase-1-safety-and-pk-data-development-candidate-selections-and-2026-outlook
12. ProQR Therapeutics. Year-end 2025 operating and financial results; about 92.4 million euros cash and runway into mid-2027, March 12, 2026. https://www.proqr.com/press-releases/proqr-announces-year-end-2025-operating-and-financial-results
13. Eli Lilly and Company. Expansion of the RNA editing collaboration with ProQR using the Axiomer platform, December 22, 2022. https://investor.lilly.com/news-releases/news-release-details/lilly-and-proqr-expand-rna-editing-collaboration
14. Treatment patterns among early inclisiran versus anti-PCSK9 antibody users, a US Komodo Health claims analysis; 12-month discontinuation 31.6 percent and proportion of days covered 0.77. Heart, Lung and Circulation, 2024. https://www.heartlungcirc.org/article/S1443-9506(24)01567-1/fulltext
15. Adherence and persistence of twice-yearly inclisiran versus twice-monthly evolocumab in Saudi Arabia, the Twice study; 9-month persistence 58.4 versus 59.8 percent. Atherosclerosis, 2025. https://www.atherosclerosis-journal.com/article/S0021-9150(25)01008-1/fulltext
16. Inclisiran efficacy in the real world, systematic review and meta-analysis; about 43 percent LDL-C reduction versus about 52 percent in trials, 2025. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12194546/
17. VICTORION-INITIATE, a randomized inclisiran-first versus usual-care implementation trial; LDL-C reduction about 60 percent versus 7 percent at day 330, goal attainment more than tripled, statin discontinuation noninferior. Journal of the American College of Cardiology, 2024. https://www.jacc.org/doi/10.1016/j.jacc.2024.03.382
18. Novartis. Leqvio (inclisiran) receives FDA approval for first-line monotherapy, describing twice-yearly, healthcare-provider-administered dosing, July 31, 2025. No home autoinjector or patient self-administration is approved to date. https://www.novartis.com/us-en/news/media-releases/novartis-twice-yearly-leqvio-inclisiran-receives-fda-approval-new-indication-enabling-first-line-use
19. U.S. Food and Drug Administration. Human Gene Therapy Products Incorporating Human Genome Editing, final guidance, January 30, 2024, Federal Register notice. https://www.federalregister.gov/documents/2024/01/30/2024-01788/human-gene-therapy-products-incorporating-human-genome-editing-guidance-for-industry-availability
20. U.S. Food and Drug Administration. Considerations for the Design of Early-Phase Clinical Trials of Cellular and Gene Therapy Products, June 2015. https://www.fda.gov/media/106369/download
21. U.S. Food and Drug Administration. Safety Assessment of Genome Editing in Human Gene Therapy Products Using Next-Generation Sequencing, draft guidance, April 2026. https://www.fda.gov/regulatory-information/search-fda-guidance-documents/safety-assessment-genome-editing-human-gene-therapy-products-using-next-generation-sequencing
22. U.S. Food and Drug Administration. Press announcement on the genome-editing next-generation-sequencing draft guidance and the agency’s innovation posture, April 2026. https://www.fda.gov/news-events/press-announcements/fda-issues-draft-guidance-genome-editing-safety-standards-advance-gene-therapy-development
23. Hogan Lovells. Summary of the FDA webinar on the finalized 2024 genome-editing guidance, including study-population and accelerated-approval recommendations. https://www.hoganlovells.com/en/publications/how-to-navigate-gene-editing-regulatory-hurdles-fda-webinar-clarifies-newly-finalized-guidance
24. Peter Marks on base editing as a potential game changer for rare and more common disease. Fierce Biotech, 2023. https://www.fiercebiotech.com/biotech/peter-marks-says-base-editing-could-be-incredible-game-changer
25. Peter Marks on traditional approval as gene therapy turns toward more common diseases. Fierce Biotech, May 2024. https://www.fiercebiotech.com/biotech/preventing-3-billion-visits-fda-year-cbers-peter-marks
26. Cell and gene therapy loses a champion at the FDA: resignation of Peter Marks as Director of the Center for Biologics Evaluation and Research, March 2025. BioPharma Dive. https://www.biopharmadive.com/news/peter-marks-cell-gene-therapy-champion-fda-departure/744026/
A Note on Supporting Independent Research
If this white paper has been valuable to you, whether it shaped your thinking, validated your conviction, or simply saved you the time of doing this work yourself, a voluntary contribution is genuinely appreciated and directly funds the next paper.
For individual investors and readers
Any amount you feel reflects the value you received is welcome and meaningful. A contribution in the range of what you might pay for a single premium research report is a thoughtful gesture that makes a real difference.
For family offices, investment funds, hedge funds, and research platforms
This paper is the caliber of work that institutional research desks bill significant retainers to produce. If your team referenced it, distributed it internally, or used it to inform a position, a suggested contribution of $1,500 reflects the professional value of the analysis, though any amount is meaningful. Your support makes it possible to continue publishing at this level without a paywall that limits the reach of the ideas. If your organization requires an invoice to process a payment, please reach out directly at bioboyscout@gmail.com and one will be provided promptly.
There is no obligation and no expectation. This is purely a thank you for work that meant something to you.
Zelle: (847) 227-7909
Thank you for reading, and for being part of a community that takes this thesis seriously.
— Robert Toczycki | BioBoyScout
Important Risks, Disclosures, & Disclaimers
The author, Robert Toczycki (aka BioBoyScout), certifies that:
· all views expressed in this white paper accurately reflect his personal opinions about the topic discussed;
· he was not compensated in any form for producing this white paper; and
This white paper is published by BioBoyScout and is intended for informational and educational purposes only. It does not constitute investment advice, a solicitation to buy or sell securities, or a guarantee of future results. The author holds a long position in Arrowhead common stock. Arrowhead Pharmaceuticals (ARWR) is a publicly traded company; investments in its shares involve material risks, including the risk of total loss. All financial projections, acquisition price estimates, and valuation analyses herein are hypothetical frameworks for analytical purposes and do not represent predictions of actual outcomes. Readers should conduct their own due diligence and consult a registered investment advisor before making investment decisions. All data cited herein were sourced from publicly available company disclosures, SEC filings, press releases, and peer-reviewed literature as of June 2026.
About the Author
Robert Toczycki is an independent analyst and registered US Patent Attorney with a JD, an Executive MBA completed at the top of his class, and a BS in Mathematics and Computer Science from the University of Illinois at Urbana-Champaign. He has a deep passion for financial analysis, particularly identifying valuation discrepancies and demonstrating them through rigorous, data-driven research and solid analytics.
Comments or questions: bioboyscout@gmail.com.
Copyright © 2026, BioBoyScout. All Rights Reserved.