
The Last Mile to the Brain
How far ARO-MAPT Has Already Been De-Risked, and the One Step That Remains

Robert Toczycki, JD, MBA
bioboyscout.com
bioboyscout@gmail.com
847.227.7909
X: @BioBoyScout
A Clinical Evidence Analysis of Why Almost Every Step of ARO-MAPT's Journey Has Already Been Proven in a Human Being, Across the Five Drugs That Each Cleared One Link of the Chain, the Single Crossing That Remains, and the Subcutaneous Brain-Delivery Platform That a Clean Readout Would Unlock.
Why this matters
Most first-in-human brain drugs are close to a coin flip. The blood-brain barrier, the biological wall that keeps most medicines out of the brain, defeats the large majority of what is sent against it, and a first clinical readout usually carries enormous uncertainty. ARO-MAPT, Arrowhead’s first wholly owned brain program, is an unusual case, because by the time its first human data arrive in the third quarter of 2026, almost every individual step in how the drug is supposed to work has already been demonstrated in a living human being, just not all by the same molecule. This note walks through those proof points in plain language, shows them in a single picture, and then points to the one step that remains genuinely unproven, and what that means. That one step is the last mile, and the last mile is the hardest mile, short in the sequence, but the most demanding leg of the journey, and the stretch the fall readout exists to test.
The journey, in plain terms
ARO-MAPT is a gene-silencing medicine. At its heart is a tiny strand of genetic material, called an siRNA, that works like an off switch for a single gene. Here the gene it switches off is the one that makes tau, a protein that builds up in Alzheimer’s disease and other brain disorders. To do its job, the drug has to complete a short journey: get into the bloodstream from a simple injection, cross the blood-brain barrier into the brain, get inside brain cells, and switch off the tau gene, which brings tau levels down. The clever part is how it crosses the wall. The drug carries its siRNA on a molecular grip, a small antibody fragment known as a Fab, that latches onto a docking point on the surface of cells called the transferrin receptor, or TfR1, which the body uses to ferry iron into the brain. The drug hitches a ride on that same system.
The question every investor really wants answered is simple: how likely is this to work in people? The most useful way to answer it is to break the journey into steps and ask, for each one, has anyone already proven this step in a human? The answer, step by step, is the heart of the case.
Five human proofs
Five different drugs, made by five different companies, have each proven a piece of ARO-MAPT’s journey in actual human beings, with two of them clearing the single hardest step, the wall itself.
Roche’s trontinemab proved the hardest-sounding part: that the transferrin-receptor grip really can carry a large molecule across the human blood-brain barrier. In Alzheimer’s patients it crossed into the brain and rapidly cleared away the sticky plaques that mark the disease. The wall can be crossed using this exact docking system.
That proof is no longer alone. In March 2026 the FDA approved tividenofusp alfa, a Denali medicine that uses the same transferrin-receptor system to carry a working enzyme from the bloodstream across the human blood-brain barrier and into brain cells, where it does its job. It cut a brain disease marker in the spinal fluid by roughly eighty to ninety percent in patients. This matters for two reasons. It is the first medicine ever approved on the strength of crossing the blood-brain barrier by this route, so the approach is now not just demonstrated but regulator-endorsed. Unlike an antibody clearing plaques outside cells, the enzyme has to get inside brain cells and function there, a closer parallel to what a gene-silencing payload must do. Two different payloads, an antibody and an enzyme, made by two different companies, have now crossed the human blood-brain barrier through this exact system.
Avidity’s del-desiran proved the next piece: that a medicine injected into the blood, routed through the same transferrin receptor, can carry a gene-silencing payload into human cells and actually switch a gene off. It lowered its target gene by roughly forty-five percent in human muscle. The approach was convincing enough that Novartis agreed to buy Avidity for about $12 billion, largely on the strength of this platform.
Alnylam’s mivelsiran proved the piece inside the brain: that a gene-silencing medicine can get into human brain cells and shut a gene down, lowering its target in the spinal fluid by roughly seventy to eighty percent. It reaches the brain by a different route, a direct injection into the spinal fluid rather than through the bloodstream, but it settles the question of whether the silencing machinery works in human neurons. It does.
Biogen’s BIIB080 proved the destination: that lowering tau itself is achievable in people, cutting tau in the spinal fluid by up to roughly half. It uses a different silencing tool than ARO-MAPT, so it does not validate the exact mechanism, but it confirms that the target Arrowhead is aiming at is a real and reachable one.
Arrowhead’s own foundation
Underneath those five human proof points sits the most directly relevant evidence of all: Arrowhead has already run the entire ARO-MAPT journey, start to finish, in monkeys. A single injection under the skin, across the blood-brain barrier, into neurons, and deep-brain tau knockdown. The five human drugs prove the individual steps are each possible in people. Arrowhead’s own primate data prove the whole chain works when assembled into one molecule, in a living primate. The human question is whether that complete chain, demonstrated in monkeys, repeats in humans.
One more piece is worth understanding, because it gives a useful measuring stick. In its monkey studies, Arrowhead compared two ways of getting the drug to the brain: the older method of injecting it into the spinal fluid, the route drugs like BIIB080 use, and its own new method of a simple shot under the skin. The spinal route makes a good benchmark, because BIIB080 has already shown, in people, that lowering tau this way works and carries over from animals to humans. In Arrowhead’s monkeys, the under-the-skin route matched or beat that spinal route, and reached deep brain regions the spinal route could not. The new route therefore cleared, in animals, a bar that a real human drug has already set. This does not prove the new route crosses the human wall. It does show that, once the drug is inside, the silencing it produces holds up against the one tau drug already proven in people.
Humans and monkeys, side by side
The same chain, shown two ways. The left column is what has been proven in humans, step by step, by drugs already in the clinic or on the market, with one step still open. The right column is what Arrowhead has proven in monkeys with ARO-MAPT itself: every step, including the one still open in humans. The contrast is the whole thesis in a single view.
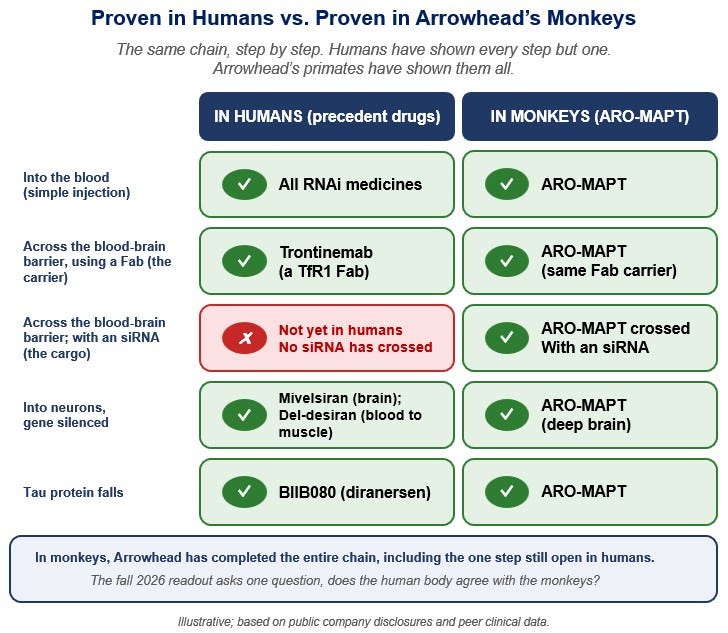
The one gap, and what it means
Look closely at the comparison above and a single honest gap appears. Every step has a human proof point except one precise junction: no one has yet shown that a medicine injected into the blood can carry a gene-silencing siRNA payload across the human blood-brain barrier and into neurons. Trontinemab carried an antibody across that wall in humans, and tividenofusp now carries an enzyme across it, approved and in patients, but neither is a gene-silencing payload. Del-desiran carried a gene-silencing payload through the blood into human cells using that same transferrin receptor, but into muscle, not across the brain’s wall. Mivelsiran silenced a gene in human brain cells, but reached them by injection into the spinal fluid, bypassing the wall entirely. The exact intersection, blood-borne delivery, across the blood-brain barrier, with an siRNA payload, has been shown in monkeys but not yet in a single human.
Notice how much narrower this gap has become. The two payloads that have already crossed the human wall, an antibody and an FDA-approved enzyme, are both far larger than an siRNA, so the carrier has proven it can haul heavier cargo than ARO-MAPT asks of it. The size of the cargo was never the problem. What remains unproven in humans is the very last part of the siRNA’s job: once across the wall and inside a brain cell, it has to slip out of the bubble that carried it in and switch the gene off. That final step has already been shown to work in people, just never in this one combination. Mivelsiran showed an siRNA can do it inside the human brain, reaching the brain by the spinal route. Del-desiran showed a blood-borne siRNA can do it through the very same transferrin receptor ARO-MAPT uses, though in muscle rather than brain. What no one has done yet is put the two together: a blood-borne siRNA, on the transferrin-receptor grip ARO-MAPT uses, doing its work across the brain’s wall. The gap is now as narrow as the human evidence can make it, one kind of cargo, at one barrier, with proof on every side of it.
There is one more piece, and for this exact step it may be the most reassuring of all. Until recently, the full journey by the new route, into the blood, across the wall, into brain cells, and the gene switched off, had been shown only by Arrowhead, in its own monkeys. That is no longer true. Independent groups have now reproduced it in monkeys, using the same transferrin-receptor system to drive gene-silencing deep into the brain: one team with an siRNA like ARO-MAPT’s, reported in a preprint, and another with a related oligonucleotide in a peer-reviewed journal. The exact route is no longer one company’s private result, though the siRNA version of it still awaits peer review.
What none of them has shown yet, Arrowhead included, is that same crossing in a human rather than a laboratory animal. These studies use animals engineered to carry the human version of the docking point, because the receptor differs from one species to the next. That is a strong stand-in for human biology, but a stand-in is what it remains, and whether the human receptor behaves in a real patient the way these animals predict is the one thing still left to settle.
It is worth knowing that Arrowhead is not the only company attempting this exact crossing. Denali, whose transferrin-receptor platform produced the approved brain-crossing enzyme described above, has its own program aimed at the same tau target, delivered from the bloodstream across the wall, and it has just entered the clinic. Newer entrants are converging on the same idea: Aerska, co-founded by a veteran of Alnylam’s early CNS siRNA delivery work, raised roughly $60 million across 2025 and 2026 to build the same kind of subcutaneous, transferrin-receptor siRNA shuttle, though its programs remain preclinical, years behind ARO-MAPT. That cuts two ways. It is validation, since serious players are convinced that reaching the brain from the bloodstream is real, and it is a reminder that the prize is contested. It does not change ARO-MAPT’s gap. It underscores that the gap is the field’s central open question, and that whoever crosses it first in humans establishes something genuinely new.
This gap matters more than its size suggests, because the blood-brain barrier is the hardest part of the whole journey, and the siRNA is the one cargo the human proof points have not yet carried across it. Within that single step, though, one half carries little doubt. The silencing that follows the crossing is the part of the process that carries over from animals to people most reliably of all, and Arrowhead’s platform has turned animal results into matching human results in the tissues it has taken into patients, so the deep monkey numbers are a fair guide to what humans would show once the drug is inside. The open question is therefore not whether the silencing works in people, but whether the drug reaches the brain to begin with. On that, the weight of evidence now leans in Arrowhead’s favor: the carrier already crosses the human wall, the silencing already carries over, and the full chain already works in monkeys, reproduced by more than one independent team. This is not a sure thing, the remaining step is genuinely the hard one and no human has yet taken it. It does mean that, for a first look at a brain drug, the odds sit better than they usually do, and on Arrowhead’s side of the line.
In the language of chess, Arrowhead has marched a pawn almost the length of the board and stands one square from promotion, the move that turns a foot soldier into a queen. A winning position, though, is not yet a win. The hardest game to win, players say, is a won one, and the conversion comes this fall.
What the readout will tell us
The first ARO-MAPT data, expected late in the third quarter of 2026, are in healthy volunteers given a single dose, and they will answer the one open question directly: did the drug cross the wall and lower tau in people, the way it did in monkeys and the way every surrounding step suggests it should.
The study is built to measure exactly that. After the injection, blood draws across the first 48 hours track the drug to confirm it reached the bloodstream and to chart how fast it peaks and clears. The brain signal comes from cerebrospinal fluid, sampled by lumbar puncture, a needle that draws fluid from the lower spine. Tau is the pharmacodynamic result everyone is watching for, the same cerebrospinal-fluid tau that fell in Arrowhead’s monkeys and that BIIB080 lowered in patients. The readout is therefore a direct measurement of the decisive step, not an indirect signal standing in for it.
That cerebrospinal fluid is sampled before dosing, for a baseline, and then at several points after, at roughly Day 75, Day 135, and Day 270. The practical meaning is worth sitting with. The first human read on tau knockdown arrives a couple of months after dosing, not on day one, and the full picture, how deep the knockdown goes and how long it lasts, is not complete until around nine months in. An early signal first, then a durability curve that fills in over the better part of a year.
One more feature of the design shapes how that signal arrives. The study is blinded: neither participants nor investigators are told who received the drug and who received the saline placebo, so the early cerebrospinal-fluid results come in as tau numbers without labels attached. Blinding hides who got what, though, not whether tau is moving. Placebo does not lower tau, so if the drug works as the monkeys predict, the data should split into two groups, a drug-sized set whose tau drops sharply from baseline and a placebo-sized set that stays flat, and that separation is itself a signal. A deep, clear knockdown would be hard to miss even before the code is broken. A weak or ambiguous one is where the blinding bites, since a small effect can hide in the noise until assignments are revealed. The clean, patient-by-patient attribution waits for that unblinding; the presence and rough size of an effect do not.
A clean result would close the last gap and turn a well-supported expectation into a proven fact. A disappointing result would say the gap was real, and that the wall, with this cargo, is harder to cross in humans than in monkeys. Either way, this is the test that matters, and it is narrow, specific, and close.
What is at stake
It is worth being clear about why a single early readout carries such weight. If ARO-MAPT crosses that last barrier in humans, the prize is not one drug. It is a proven, repeatable way into the brain. The same delivery that carries this siRNA across the wall, a simple shot under the skin, could then be aimed at one brain gene after another, which is why a clean result would validate a platform, not a product. The brain has been the hardest organ in the body to drug, walled off from exactly the gene-silencing medicines that have already proven themselves in the liver. A simple injection that reliably silences a chosen gene in the brain would turn a long list of once-unreachable targets into a pipeline. That is the real stake, and it rests on the delivery question the fall readout tests, not on any later one. The platform is validated the moment the crossing is, whether or not any single drug goes on to prove it treats a disease.
Tau itself is no small target. It sits at the center of Alzheimer’s and a family of related brain disorders driven by the same protein, an enormous unmet need and, if the biology holds, a commercial opportunity to match. That upside, though, rests on two separate questions, not one: whether the drug reaches and silences tau in people, which the fall readout tests, and whether lowering tau meaningfully changes the course of Alzheimer’s, which no one has yet proven and which years of patient data will decide. The delivery result would be a landmark on its own, and the platform it unlocks larger still. The therapeutic payoff is a further bet placed on top of both.
There is a market consequence worth naming. Arrowhead’s CNS pipeline is, for now, priced largely as option value: a promising route to the brain that no human result has yet confirmed. A clean readout would not re-rate one drug so much as the platform behind it, because proof of the crossing converts that option value into an expectation, and does so across every brain program the same delivery could carry. The size of any such move depends on what the stock already discounts, which is beyond the scope of this note. The direction, if the crossing is shown, is not hard to reason out.
The bottom line
Every step of ARO-MAPT’s journey has already been walked in a human being, just not all by the same molecule, and not yet across the one wall that matters most.
That is the whole case in a sentence. This is not a leap into the dark. It is a short step across a single, well-lit gap, onto ground that five other drugs have already proven can hold weight, with Arrowhead’s own monkeys having made the full crossing first. The science is no longer asking whether any of this can work, because each piece already does, in people. It is asking one question, and only one: can a molecule injected into the blood carry its silencing payload across the human blood-brain barrier and into a neuron? Monkeys have already said yes. This fall, humans will answer.
A Note on Supporting Independent Research
If this note has been valuable to you, whether it shaped your thinking, validated your conviction, or simply saved you the time of doing this work yourself, a voluntary contribution is genuinely appreciated and directly funds the next paper.
For individual investors and readers
Any amount you feel reflects the value you received is welcome and meaningful. A contribution in the range of what you might pay for a single premium research report is a thoughtful gesture that makes a real difference.
For family offices, investment funds, hedge funds, and research platforms
This paper is the caliber of work that institutional research desks bill significant retainers to produce. If your team referenced it, distributed it internally, or used it to inform a position, a suggested contribution of $1,000 reflects the professional value of the analysis, though any amount is meaningful. Your support makes it possible to continue publishing at this level without a paywall that limits the reach of the ideas. If your organization requires an invoice to process a payment, please reach out directly at bioboyscout@gmail.com and one will be provided promptly.
There is no obligation and no expectation. This is purely a thank you for work that meant something to you.
Zelle: (847) 227-7909
PayPal: paypal.me/bioboyscout
Thank you for reading, and for being part of a community that takes this thesis seriously.
— Robert Toczycki | BioBoyScout
Important Risks, Disclosures, & Disclaimers
The author, Robert Toczycki (aka BioBoyScout), certifies that:
all views expressed in this note accurately reflect his personal opinions about the topic discussed;
he was not compensated in any form for producing this note; and
he has not received and does not receive compensation from Arrowhead Pharmaceuticals.
This note reflects the author’s personal opinions, is for informational purposes only, and is not investment advice. Comparisons to other companies’ drugs are illustrative of scientific precedent and do not imply equivalence of outcome. Clinical figures are drawn from public company disclosures and peer-reviewed sources. It does not constitute investment advice, a solicitation to buy or sell securities, or a guarantee of future results. The author holds a long position in Arrowhead common stock. Arrowhead Pharmaceuticals (ARWR) is a publicly traded company; investments in its shares involve material risks, including the risk of total loss.
About the Author
Robert Toczycki is an independent analyst and registered US Patent Attorney with a JD, an Executive MBA completed at the top of his class, and a BS in Mathematics and Computer Science from the University of Illinois at Urbana-Champaign. He has a deep passion for financial analysis, particularly identifying valuation discrepancies and demonstrating them through rigorous, data-driven research and solid analytics.
Comments or questions: bioboyscout@gmail.com.
Copyright © 2026, BioBoyScout. All Rights Reserved.